


 720-777-0123
720-777-0123






Key takeaways
-
Infantile scoliosis signs include differences in appearance of shoulder blades, shoulder height or rib prominence.
-
A pediatric spine specialist should perform radiographs to confirm and track the progression of infantile scoliosis and an MRI should be considered if the patient exhibits signs of a neural tube defect.
-
Spinal fusion surgery in young patients is being replaced by spinal casting at specialty centers due to the risk for respiratory compromise later in life as a result of surgery.
Infantile scoliosis is a relatively common diagnosis, but the true incidence is unknown. Most mild cases go undetected. Approximately 80-90% of identified cases resolve on their own with normal growth.
Diagnosing infantile scoliosis
Signs of infantile scoliosis include differences in shoulder blade appearance from side to side, shoulder height difference and prominent ribs on one side of the body.
Radiographs (X-rays) are recommended for children with suspected scoliosis. If your radiology site is not accustomed to doing spinal radiographs on infants, it is recommended to defer these until an evaluation is done by a pediatric spine specialist.
If there is a hairy patch or a sacral dimple that does not have a visible floor, evaluation of the spinal axis by ultrasound or MRI may be recommended to evaluate for neural tube defect. An ultrasound can be done without sedation, but generally only before the age of 3 to 6 months. After six months, the posterior spine elements have mineralized which distorts the ultrasound image. MRI generally requires sedation for infants, but some infants can undergo MRI without sedation if they are given a feeding and then fall asleep for the scan.
Observing infantile scoliosis
Treatment options for infantile scoliosis are typically non-surgical. In most cases, the scoliosis will resolve with normal muscular development. Until infantile scoliosis is resolved, it's important for the orthopedic team to observe the patient and take radiographs as indicated.
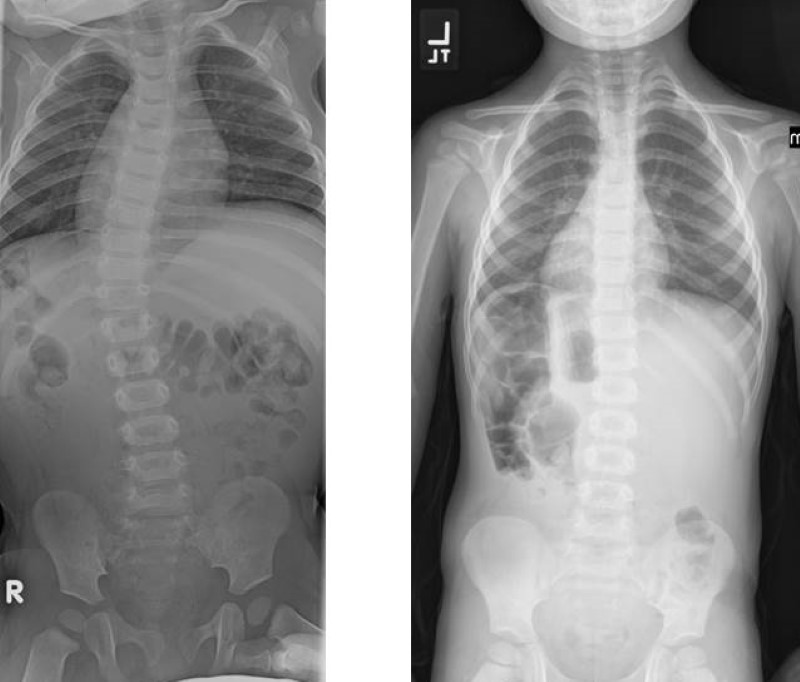
Radiographs can help identify patients at risk for progression of scoliosis based on the magnitude of the scoliosis and the amount of associated chest rotation. Resolving infantile scoliosis generally has little chest rotation while progressive infantile scoliosis has a greater amount of chest rotation. This is clinically seen as more asymmetry of the rib cage. On radiographs this appears as asymmetric angulation of the ribs as they take off from the spine.
Treatment for infantile scoliosis
For cases that fail observation or have a high risk of progression, the mainstay of treatment is serial spine casting. Casting has been used for infantile scoliosis for many decades, but was largely abandoned in the late 1990s due to enthusiasm for early surgical correction with spinal fusion. Unfortunately, children having early spinal fusion often develop significant respiratory compromise as adults. This is due to restrictive lung disease from an abnormally short trunk caused by the surgery.
Experts often suggest MRIs for children with progressive infantile scoliosis because there is a 10-15% incidence of associated spinal axis abnormalities (e.g., Chiari malformation, syrinx, spinal cord tumor, tethered spinal cord).
Spine casting is done under general anesthesia with a skilled team experienced in proper casting technique. Improper casting can be ineffective at controlling scoliosis, and in worst cases, it can cause further chest wall restriction and skin pressure sores.
In the past, casting was mainly done only for children with idiopathic scoliosis (no known cause for scoliosis). Now, more pediatric orthopedic specialists also use casting for non-idiopathic cases for children with congenital spinal malformations to delay surgery. Casting should be done only at centers like the Spine Program at Children's Colorado with pediatric expertise in the treatment of infantile scoliosis to maximize effectiveness and minimize risks.
Contact us
Email: spine@childrenscolorado.org
Phone: 720-777-6962


